Center for Community Health, UCLA Wilshire Center
10920 Wilshire Blvd., Suite 350, Room 350-46 (Conference Room)
mHealth solutions have been proposed to address healthcare system inefficiencies in resource-poor settings, especially for home-based HIV testing and counseling (HTC) programs. The transfer of rapid diagnostic testing and health information from the field to the clinic is crucial for the success of home-based HTC programs; mHealth solutions have been pilot-tested. Yet wide-scale mHealth adoption has not occurred. Even as infrastructure barriers decrease, a need to better understand perceived adoption barriers by stakeholders remains. We conducted focus group discussions (FGD) in South Africa in 2016 with 10 field staff from a home-based HTC program, 12 community health workers (CHWs) and 10 persons living with HIV. Key informant (KI) interviews were conducted with five health officials. Perceptions about current home-based HTC practices, future mHealth systems and the use of biometrics for patient identification were discussed and will be presented during the seminar. In addition, I will discuss how qualitative findings are being used to inform the development of future mHealth systems.
The CHIPTS’ Methods Core hosts a monthly seminar series, which are one-hour workshops on research and statistical methods. The seminars are open to HIV researchers, faculty, students, and community. To see previous seminars, check out the Methods Seminar tag or you can find seminar videos on our Youtube Channel! This series is hosted by the Center for HIV Identification, Prevention, and Treatment Services (CHIPTS) and made possible by funds from the National Institute of Mental Health (MH058107).
Erik Storholm, PhD is a core affiliate in the Combination Prevention Core at CHIPTS. He is an Associate Behavioral Scientist at the RAND Corporation and a Licensed Clinical Psychologist. He is also a scholar in the UCLA HIV/AIDS, Substance Abuse and Trauma Training Program and an affiliate research scientist in the Department of Research and Evaluation at Kaiser Permanente Southern California. In addition to conducting research, Erik maintains an active private practice in West Hollywood, CA where he sees patients.
Erik’s work in health disparities began 15 years ago in San Francisco when he was volunteering at HIV/AIDS service organizations conducting outreach interventions to help document and reduce the spread of the virus among high-risk minority communities. This work stimulated his interest in understanding human behavior, decision-making, structural sources of inequality, and propelled his interest in health disparities research. Over the years, he has had the privilege of working with hundreds of participants spanning the spectrums of race, ethnicity, class, age, sexual orientation, and HIV diagnosis status. As he listens to his participants put their lives into words, Erik hears true testaments of resiliency and strength, as well as, countless stories of trauma, loss, discrimination, disempowerment, and unequal access to healthcare, employment, and education. These health disparities that fall along racial and ethnic lines have been impossible to ignore. It is this work that has fostered Erik’s desire to dedicate his life’s work to conducting health disparities research that promotes equality, empowerment, social justice, and equal opportunity while reducing health disparities among members of marginalized communities. This research has underscored his commitment to unmasking the integral role of socially produced ills such as stigma, discrimination, and lack of access to resources in the development and exacerbation of mental health problems, substance use, and HIV/STI disparities.
Erik recently completed a study assessing changes in risk perception and behavior, substance use, and medication adherence among young sexual minority men prescribed pre-exposure prophylaxis (PrEP) to prevent HIV infection. His primary research interests are all within the area of health disparities, specifically in clinical interventions that focus on mental health, substance abuse, and the prevention of HIV/STI transmission among high-risk minority populations. Currently, Erik is leading several NIH-funded projects in the area of combination biobehavioral HIV prevention intervention design and evaluation, PrEP uptake and adherence among minority communities.
Erik enjoys traveling, hiking, eating great food, and exploring new neighborhoods in Los Angeles. He is also an avid snowboarder and tries to hit the slopes whenever he can. He is active in psychological communities and spends most of his free time with his best friends in Los Angeles and New York City.
Each month, we’re featuring a member of our CHIPTS family and their work! To see past spotlights, check them out on the spotlights page and make sure to check back to see who we feature next!
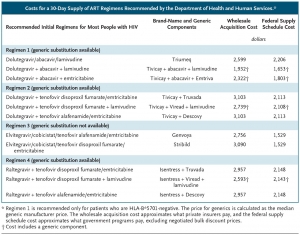
Combination antiretroviral therapy (ART) has dramatically improved survival rates among people with HIV and is a mainstay of HIV prevention; evidence shows that durable viral suppression prevents the transmission of infection. In addition, preexposure prophylaxis (PrEP) is an emerging approach to preventing HIV acquisition for certain high-risk groups. Generic ART medications offer the potential for treating and preventing HIV with fewer resources. Generic versions of lamivudine, abacavir, and efavirenz became available in the United States within the past 6 years at prices lower than their brand-name counterparts, a generic version of PrEP (emtricitabine and tenofovir disoproxil fumarate) was approved in 2016, and generic versions of tenofovir disoproxil are expected later in 2018. Yet most of the discussion about the availability of generic HIV drugs focuses on low- and middle-income countries.
Costs for a 30-Day Supply of ART Regimens Recommended by the Department of Health and Human Services.
ART accounts for 60% of the projected $326,500 discounted lifetime medical cost of HIV treatment in the United States.1 A 2013 study estimated nearly $1 billion in savings in the first year if all eligible U.S. patients for whom brand-name was prescribed efavirenz at the time (when it was a component of a leading ART regimen) switched to a regimen with generic efavirenz.2 Our analysis of four regimens currently recommended by the Department of Health and Human Services (HHS) shows in more detail the potential cost savings associated with switching to generic regimens (see table). For example….
To continue reading, please visit The New England Journal of Medicine websitehere.
Differences found by Age, Gender, Race/Ethnicity, and Geographic Region
LOS ANGELES — Despite large increases in PrEP use across California, a new study funded by the California HIV/AIDS Research Program finds sharp differences in uptake by age, gender, race/ethnicity and geographic region. In this first look at PrEP prescription data among beneficiaries of California’s Medicaid program, Medi-Cal, researchers were able to document that from 2012 through 2016, PrEP uptake was lower among Blacks, Hispanics, women, and people between the ages of 13-24. Disparities were also identified with regard to geographic region. Uptake was highest in San Francisco County, followed by San Diego and Los Angeles Counties.
Key findings include:
Rates of PrEP uptake are much lower for the youngest age group, ages 13-24, than for those ages 25-34 or 35-44 years.
Rates of uptake for women and those ages 65 and older are slow to rise and appear to have be leveling for women.
Rates of PrEP uptake for non-Hispanic Blacks are consistently lower than observed for Whites; yet new diagnoses among Blacks/African Americans are over 4 times that of Whites.
Hispanics have the lowest overall rates of PrEP uptake even though HIV rates for Hispanics in the state are 1.5 times those of Whites.
Increased rates of PrEP uptake were found in the 3 largest counties and both rural and urban areas. The steepest increase was found in San Francisco County which, in the second half of 2016, outpaced uptake in Los Angeles and San Diego by more than 5 times.
Senior author, Nina Harawa, PhD, MPH of UCLA and Charles Drew University shared, “Even when accessible, PrEP’s reach into communities most impacted by HIV continues to fall short. If increased PrEP use is a key strategy for California’s plan to get to zero new infections, it is critical that we examine these disparities and remove social and logistical barriers to PrEP use for young and old, women as well as men, and black and brown communities.”
These findings echo data from Gilead Pharmaceuticals, the maker of the currently approved PrEP regimen, Truvada®. In 2017, Gilead noted that PrEP uptake varies by demographic characteristics, risk group, and region in the U.S. This work also underscores findings from a prior study by the Southern California HIV/AIDS Policy Research Center that identified racial/ethnic disparities in PrEP uptake among gay, bisexual, and other men who have sex with in California and indications of a significant association between higher income and PrEP usage.
Los Angeles County released their HIV/AIDS Strategy for 2020 and Beyond in December 2017. For more information on the Strategy, please download the pdf below or visit the LA County HIV website.
More than 36 years ago, Los Angeles County (LAC) was among several major metropolitan areas in the United States to report the first documented cases of what is now known as HIV/AIDS. Since that report in June 1981,1 an initial group of 5 cases in Los Angeles County would grow to nearly 90,000 diagnosed cases of HIV or AIDS. Almost 30,000 persons diagnosed with HIV/AIDS in Los Angeles County have died. Over that same time, the number of annual new HIV infections reported in LAC would rise to a peak of more than 6,500 and slowly decline to the 1,850 new HIV infections estimated for 2017. The number of residents with undiagnosed HIV infection would grow to more than 15,500 in the early 2000s and slowly decline to an estimated 8,900 (or about 14% of all persons living with HIV) today. There has been steady, deliberate progress, but a public health imperative calls on all of us to do more.
Today, more than 60,000 persons live with HIV in Los Angeles County, and many people living with HIV are effectively managing their infection (as measured by the undetectable levels of HIV in their bloodstream, or viral suppression) with the use of highly active anti-retroviral therapy (ART). Many of our most marginalized and disenfranchised residents can achieve viral suppression through the combined access to lifesaving treatment and a menu of services that improves health system navigation and access (including to physical, mental and oral health services, housing stability, food and nutrition services, substance use treatment, care coordination and transportation services). For tens of thousands of persons in Los Angeles County with either undiagnosed HIV infection or who have been diagnosed, but for a multitude of complex reasons have unmanaged HIV infection, the benefits of scientific progress, public health action, and clinical intervention will be realized if they are diagnosed, linked to care, and treated in a timely manner.
Every day, I wake up and take a little blue pill that empowers me. It’s been nearly 3 years since I made the decision to start pre-exposure prophylaxis, better known as PrEP. PrEP is a daily pill that when taken consistently reduces the risk of acquiring HIV by over 90%. Over the years, I’ve learned some valuable lessons about taking PrEP that I’d like to share as we observe National Black HIV/AIDS Awareness Day.
Lesson #1: You don’t know what you don’t know. So Ask!
Much like many other black gay/bisexual men, when I first began considering PrEP, I had awareness that PrEP existed but I didn’t have enough knowledge to make an informed decision about whether or not it was the right choice for me. Even with limited knowledge, I got motivated. My lack of knowledge would not be my Achilles heel. So, I researched reliable sources, engaged friends and colleagues who were taking PrEP about their experiences, and had a conversation with my primary care provider about whether or not PrEP was right for me. Though my primary care provider had some knowledge, he wasn’t comfortable prescribing the pill to me. He was able to refer me to an Infectious Disease (ID) provider within my network. After meeting with my ID provider, I found that asking questions to a provider who I trusted improved my understanding and quieted any fears I had about PrEP.
Providers can take steps to become more knowledgeable about PrEP through webinars, in-person trainings, and guidelines [PDF, 868 KB] provided by the Centers for Disease Control and Prevention (CDC). There’s even a PrEP line providers can call for guidance! There is also a free, accredited, online continuing education module for healthcare providers about PrEP supported by the Health Resources and Services Administration’s HIV/AIDS Bureau.
The power of knowledge shouldn’t be limited to providers though. Patients have knowledge to share with friends and family as well as with their providers who, like mine, sometimes need to learn more about PrEP. Widespread lack of awareness of this powerful HIV prevention tool shouldn’t be the norm
Lesson #2: PrEP is an option, but not the only one.
CDC estimates that more than 1.2 million people are indicated for PrEP. Based upon Federal guidelines, recommendations include anyone who:
is HIV-negative and in an ongoing sexual relationship with an HIV-positive partner.
isn’t in a mutually monogamous* relationship with a partner who recently tested HIV-negative, and is a . . .
gay or bisexual man who has had anal sex without using a condom or been diagnosed with an STD in the past 6 months, or
heterosexual man or woman who does not regularly use condoms during sex with partners of unknown HIV status who are at substantial risk of HIV infection (for example, people who inject drugs or women who have bisexual male partners).
* Mutually monogamous means that you and your partner only have sex with each other and do not have sex outside the relationship.
No matter where you fit in, it’s important to recognize this: One size doesn’t fit all. In my prior work in HIV prevention and treatment, I’ve never told clients: “You should do this.” I’ve always been in the business of offering options, not directives. We have to understand that HIV prevention is a lot like a buffet. Equipped with knowledge about their options, people are free to pick and choose (or not choose) which prevention method(s) work for them. Some individuals are not comfortable with or confident about taking a pill everyday. That’s ok. Instead, they can choose to rely on condoms, treatment as prevention, or other effective HIV prevention methods. That’s ok, too. Do what works for you. I believe that no one should be shamed for making choices that empower them.
To see the other points that Jamal Refuge makes, visit the HIV.gov website here.
February 2, 2018, CDC – Non-Hispanic blacks/African Americans (blacks) represent 12% of the U.S. population.* However, in 2014 an estimated 43% (471,500) of persons living with diagnosed and undiagnosed human immunodeficiency virus (HIV) infection were blacks (1). In 2016, blacks accounted for 44% of all new HIV diagnoses (2). Although antiretroviral therapy (ART) prescriptions among persons in HIV care increased overall from 89% in 2009 to 94% in 2013, fewer blacks than Hispanics or Latinos (Hispanics) and non-Hispanic whites (whites) were on ART and had a suppressed viral load (<200 HIV RNA copies/mL) in their most recent viral load test result (3). Blacks also might be less likely to have sustained viral suppression over time and to experience longer periods with viral loads >1,500 HIV RNA copies/mL, a level that increases the risk for transmitting HIV (4–7). National HIV Surveillance System (NHSS) data are among those used to monitor progress toward reaching the national goal of reducing health disparities. CDC analyzed NHSS data to describe sustained viral suppression and transmission risk potential by race/ethnicity. Among 651,811 persons with HIV infection diagnosed through 2013 and who were alive through 2014 in 38 jurisdictions with complete laboratory reporting, a lower percentage of blacks had sustained viral suppression (40.8%), than had Hispanics (50.1%) and whites (56.3%). Among persons who were in care (i.e., had at least one viral load test in 2014) and had not achieved sustained viral suppression in 2014, blacks experienced longer periods (52.1% of the 12-month period) with viral loads >1,500 copies/mL, than did Hispanics (47.2%) and white (40.8%). Blacks aged 13–24 years had the lowest prevalence of sustained viral suppression, a circumstance that might increase transmission risk potential. Strengthening interventions that improve access to ART, promote adherence, and address barriers to clinical care and supportive services for all persons with diagnosed HIV infection is important for achieving the national goal of reducing health disparities…
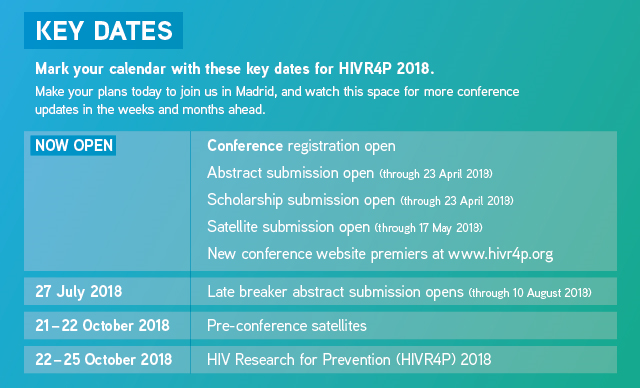
Abstract submission, scholarship applications and registration for HIVR4P 2018 open today!
This is a big day on the HIVR4P 2018 calendar. Abstract submission, scholarship applications and conference registration for HIVR4P 2018 are all now officially open. Also premiering today: the fully updated HIVR4P 2018 website, with more information about the conference program, venue and host city. Visit our website and make your plans to join us for HIVR4P 2018, 21–25 October 2018 at the Madrid Marriott Auditorium Hotel.
Today through 23 April, HIVR4P is accepting abstract submissions in 29 research categories, covering every dimension of HIV prevention research…from Antibody Functions to the Microbiome to Treatment as Prevention, and every aspect in between. Through both abstract and non-abstract driven sessions, HIVR4P supports cross-fertilization between every field of HIV prevention research, while also providing a unique venue to discuss the findings, questions and priorities specific to each.
HIVR4P’s outstanding Abstract Review Committee comprises close to 100 members representing twenty countries and every field of HIV prevention research. HIVR4P 2016 received 934 abstract submissions, and accepted 144 for oral presentation and 575 as posters. Help us continue a growing tradition in excellence by submitting your research to HIV Research for Prevention, the world’s only scientific conference dedicated exclusively to all forms of biomedical HIV prevention, including vaccines, treatment as prevention, microbicides, PrEP and new and emerging forms of prevention.
Scholarships
As part of our commitment to ensuring global participation in the meeting, HIVR4P 2018 will award 200 full scholarships (travel, registration & hotel) and 100 registration-only scholarships to outstanding young investigators and community representatives. Research scholarships are open to graduate students, junior faculty and post docs submitting an abstract to the conference. Learn more and apply for a scholarship to HIVR4P 2018 here.
Registration
Register early to ensure your place at HIVR4P 2018 and save. Full information on conference registration can be found here.
And be sure to visit the new HIVR4P 2018 conference website, which will be updated regularly with program information, travel tips, interviews and news from the conference headquarters. Check back often for updates from HIVR4P 2018.
Conference program details…coming soon!
Just days ago, approximately 40 members of the HIVR4P 2018 Program Organizing Committee (POC) met in New York to organize the plenary, roundtable and symposia sessions that are a critical component of the diverse HIVR4P program.
Watch their website and future editions of their newsletter for details on the conference program, including daily plenary sessions featuring the leading global voices in HIV prevention research, and roundtables and symposia on topics such as barriers and facilitators of transmission at the mucosa; innate and adaptive immune responses in HIV dissemination; early events in establishment of HIV infection; developing policy for clinical use of PrEP; accelerating product introduction for epidemic impact; passive antibody infusion; induction of broadly neutralizing antibodies through vaccination; designing and implementing the next generation HIV prevention trials; and many other pressing topics from the field.
Did you know that registration fees pay only a small portion of what it costs to hold HIVR4P?
With more than 300 full and partial scholarships for early-career investigators, community leaders and journalists, a fully webcast program and our commitment to ensuring global participation from every field of HIV prevention research, HIVR4P presents a uniquely inclusive opportunity to advance every aspect of the global HIV response.
Our partners from government, philanthropy and the private sector make much of this work possible. Learn more about the benefits of partnership, and consider joining these leaders who make HIVR4P a truly global effort to advance HIV prevention. For more information, please visit our Sponsorship page.
Want to get your organization’s message out, highlight new approaches or opportunities in HIV prevention research or delivery, or simply provide a more in-depth focus on prevention than a regular conference presentation will allow?
A satellite session at HIVR4P 2018 provides the perfect opportunity to dive deep into the issues that most concern your organization, shine a light on new prevention strategies, highlight the needs of key populations or address any other aspects of the epidemic that deserve extra attention.
Satellite sessions at HIVR4P are held on 21 and 22 October, immediately before the main program, and take place in the conference venue—guaranteeing you access to more than 1,400 researchers, policy makers, funders and advocates from around the world attending HIVR4P.
Applications for satellite sessions at HIVR4P 2018 are being accepted through 17 May. Details and a link to the satellite application page are available here.
Sign up for updates from HIVR4P 2018
Keep on top of the conference news and receive regular updates from HIVR4P 2018 by signing up here. And watch this space for more updates from HIV Research for Prevention (HIVR4P) 2018.
A new report has estimated that almost 700,000 LGBT adults (ages 18-59) in the U.S. have received conversion therapy while an estimated 20,000 LGBT youth in the U.S. (ages 13-17) will receive conversion therapy from a licensed health care professional before the age of 18. Conversion therapy is meant to change the sexual orientation, gender identity, or gender expression of an individual, rooted in the idea that being LGBT is abnormal.
The new report out of The Williams Institute, UCLA School of Law dives into the history of conversion therapy that has been in practice for over a century in the United States, current perspectives of professional health associations and the public opinion, as well as current laws in place. There are currently nine states and the District of Columbia that has legally limited the use of conversion therapy: California, D.C., Illinois, New Jersey, Vermont, Oregon, Connecticut, Rhode Island, Nevada, and New Mexico with the latter four states passing bans in 2017.
January 26, 2018 – Last Friday, the Center for HIV Identification, Prevention, and Treatment Services (CHIPTS) hosted its 2018 HIV Next Generation Conference (Next Gen) on UCLA campus. Opening remarks from Drs. Steve Shoptaw and Dallas Swendeman energized the 128 attendees that filled the room, followed by a dynamic plenary presentation given by Dr. Raphael Landovitz, who presented on the state of the science and future direction of pre-exposure prophylaxis (PrEP).
CHIPTS faculty Drs. Li Li and Dallas Swendeman engaging with poster presenter Chiao-Wen Lan.
Throughout the day, six trainees gave oral presentations of their research projects and received thought provoking questions from the audience, which ranged from researchers, community providers, faculty members, and other students. Additionally, thirteen trainees showcased their work during the poster session which lend to many lively conversations allowing undergraduate, graduate, and postdoctoral researchers to network with faculty and the community.
(L to R) Natalie Sanchez, Hilda Sandoval, and Ramon Garcia of AltaMed Services respond to questions from the audience regarding Sin Vergüenza Season 3.
In addition, the conference featured a community panel that included Ms. Natalie Sanchez, Dr. Hilda Sandoval, and Mr. Ramon Garcia from AltaMed, who presented on the telenovela series, Sin Vergüenza Season 3. In their presentation, they discussed the impact of using visual media to educate and address stigma, homophobia, transphobia, and addiction among those living with HIV and their communities.
Wendy Garland from LAC DHSP talking about LA County’s new HIV strategy and other programs by DHSP.
Ms. Wendy Garland of the Los Angeles County Division on HIV and STD Programs (DHSP) gave the afternoon plenary presentation. She provided an overview of the Los Angeles County HIV/AIDS Strategy for 2020 and Beyondinitiative (https://www.lacounty.hiv/) as well as other key programs led by DHSP. In addition to sharing the priorities for HIV and STD prevention and treatment for Los Angeles County, she highlighted a number of opportunities for collaboration, which received excitement from many conference attendees.
Dr. Eric Rice of USC speaks on artificial intelligence to enhance HIV prevention.
Later in the afternoon, members of the UCLA Center For AIDS Research Health Disparities Core, which included Drs. Lee Klosinski, Eric Rice, Ian Holloway, and Ayako Miyashita, tackled the theme of health disparities. Dr. Klosinski provided context and background in establishing the Core and emphasized the importance of addressing health disparities in key populations impacted by HIV. Dr. Rice from the University of Southern California presented on the use of artificial intelligence to enhance HIV prevention programs targeting homeless adolescents, while Dr. Holloway and Ms. Miyashita presented on their mobile-based HIV intervention aimed at increasing linkages to HIV, social work, and legal services for HIV-positive African American young men who have sex with men.
At the end of the day, attendees voted for the best scientific oral and poster presentations. Doctoral student, Sid Jordan, won the best scientific oral presentation with his work on “Gender Diversity in Prevention: Findings Transmasculine Sexual Health and Reproductive Justice Survey” and undergraduate researcher, Joshua Cohen, received the best poster award for “Relationships Between Substance Use, Nicotine Use, and HIV in Ethnic Men Who Have Sex with Men.” The conference proved to be a full day of science, networking, and learning.
The winners of Best Oral Presentation, Sid Jordan, and Best Poster Presentation, Joshua Cohen, holding their certificates.
Below are PDF version of the event program and presentation slides. You can find ourhighlight gallery from the day on our Facebook page.
Steve Shoptaw, PhD
Director, CHIPTS
Professor, UCLA Departments of Family Medicine and Psychiatry and Biobehavioral Science
Vice Chair, Research in Family Medicine
Dallas Swendeman, PhD, MPH
Associate Professor, UCLA Department of Psychiatry and Biobehavioral Sciences
Development Core Director, CHIPTS
Moderated by Thomas Coates, PhD
Distinguished Professor of Medicine, UCLA David Geffen School of Medicine
Michael and Sue Steinberg Professor of Global AIDS Research
Director, UCLA Center for World Health
Global HIV Director, CHIPTS
Moderated by Cathy Reback, PhD
Senior Research Scientist, Friends Research Institute, Inc.
Executive Director, Friends Community Center
Combination Prevention Core Director, CHIPTS
LINX LA Study - Slides
Ayako Miyashita, JD
Assistant Adjunct Professor, Luskin School of Public Affairs, Department of Social Welfare
Associate Director, UCLA California HIV/AIDS Policy Research Center
Ian Holloway, PhD, MSW, MPH
Assistant Professor, UCLA Luskin School of Public Affairs, Department of Social Welfare
Prevention
Moderated by Norweeta Milburn, PhD
Professor-in-Residence, UCLA
Department of Psychiatry and Biobehavioral Sciences
Director, UCLA Center For AIDS Research Health Disparities Core
Core Scientist, CHIPTS
Sid Jordan, JD
Gender Diversity in Prevention: Findings Transmasculine Sexual Health and Reproductive Justice Survey
Steve Shoptaw, PhD
Director, CHIPTS
Professor, UCLA Departments of Family Medicine and Psychiatry and Biobehavioral Science
Vice Chair, Research in Family Medicine
Dallas Swendeman, PhD, MPH
Associate Professor, UCLA Department of Psychiatry and Biobehavioral Sciences
Development Core Director, CHIPTS
We would like to thank the members of the Conference Planning Committee for their countless hours in planning and organizing this conference including: Ron Brooks, Isabelle Chu, Roger Detels, Nina Harawa, Uyen Kao, Raphael Landovitz, Sung-Jae Lee, Norweeta Milburn, Steve Shoptaw, Stephanie Sumstine, and Dallas Swendeman.
Also, we would like to thank the generous volunteers who helped with today’s event including: Jennifer Baughman, Sandra Cuevas, Marcos Garcilazo-Figueroa, and Diane Tan.

 W. Scott Comulada, Dr.P.H.
W. Scott Comulada, Dr.P.H.