Registration Link: https://goo.gl/forms/2Tw0nwIArUVdB4y93
You can see the Agenda below or download it and parking instructions here:
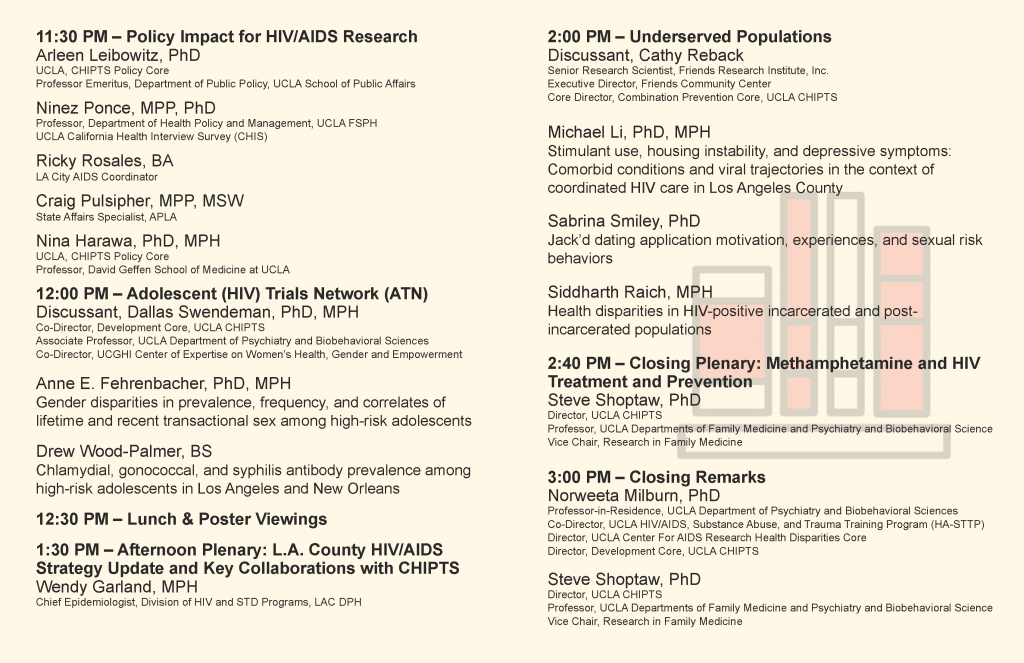
2019 HIV Next Generation Conference - Agenda
[Download not found]
![]()


Registration Link: https://goo.gl/forms/2Tw0nwIArUVdB4y93
You can see the Agenda below or download it and parking instructions here:
2019 HIV Next Generation Conference - Agenda
[Download not found]
![]()

Latoya Small, MSW, PhD, is an Assistant Professor in the Luskin School of Public Affairs, Department of Social Welfare and is part of the Policy Impact Core at CHIPTS. Her research examines how social determinants of health are associated with HIV treatment outcomes in both the U.S. and Sub-Saharan Africa. More specifically, her work aims to develop evidence-based interventions focused on HIV and behavioral health among women and children, within the context of poverty. Currently, Latoya has a project that is looking at how poverty, stress, parenting, and mental health factors impact adherence to HIV medical services among Black women in urban Los Angeles.
Prior to her research career, she provided direct clinical services for almost 10 years. As a clinical social worker, Latoya provided mental health services to children and families in her hometown of South Los Angeles and later worked with persons who had severe and persistent mental illness, in a state psychiatric facility. Her international social work began when she worked with children in foster care in the United Kingdom. Afterwards, she moved to South Africa where she gained her first experience in conducting HIV research among vulnerable youth. These experiences laid the foundation for her health disparities research on HIV and behavioral health.
In 2015, Latoya received funding from the International AIDS Society to lead a two-year study entitled, “VUKA EKHAYA: A Take Home Family Intervention to Improve Adherence and Reduce Behavioral Risk among Perinatally HIV-Infected Youth.” This intervention was informed by community-based participatory research and aimed to address the need for empirically-informed and sustainable HIV care approaches for perinatally HIV-infected youth in Durban, South Africa. The study was a culturally-informed, cartoon-based family intervention designed for low-literacy populations, targeting mental health and risk behaviors of seropositive underserved youth.
Currently, Latoya is conducting a CHIPTS-funded pilot study, examining the relationship between mental health and treatment adherence for African American women living with HIV in urban Los Angeles. Charged by the recent policies that perpetuate inequities and health disparities faced by transgender people, Latoya adapted her research to include the needs of the transgender women and children, to better understand their unique experiences. This led her to receiving a UCLA junior faculty award to explore whether exposure to violence, discrimination, and health differ by race among transgender persons across different regions of the United States.
When she is not working, Latoya enjoys reacquainting herself with Los Angeles beaches, exploring taco stands, and hiking in Griffith Park.
Each month, we’re featuring a member of our CHIPTS family and their work! To see past spotlights, check them out on the spotlights page and make sure to check back to see who we feature next!
The CHIPTS’ Methods Core hosts a monthly seminar series, which are one-hour workshops on research and statistical methods. The seminars are open to HIV researchers, faculty, students, and community. To see previous seminars, check out the Methods Seminar tag or you can find seminar videos on our Youtube Channel! This series is hosted by the Center for HIV Identification, Prevention, and Treatment Services (CHIPTS) and made possible by funds from the National Institute of Mental Health (MH058107).


The HIV Prevention Trials Network are currently accepting applications for their HPTN Scholars Program.
Applications for US domestic scholars are due on January 25, 2019. Applications for international scholars are February 22, 2019. See more details below or visit the official HPTN website.
For more information about the HPTN Scholars Programs, please contact Ehamilton@fhi360.org.
HPTN investigators who are based at UCLA and might be able to serve as mentors include: Raphael Landovitz MD, MSc, Steve Shoptaw, PhD, Jesse Clark, MD, Tom Coates, PhD, and others. Please feel free to contact them directly.
Application materials for the HPTN Scholars program are available for early-career minority investigators who wish to collaborate with the HPTN in the development and implementation of our research agenda.
Submission Deadlines:
U.S. Domestic Scholars: Initial proposal drafts are due January 11, 2019; full applications are due January 25, 2019.
International Scholars: Initial proposal drafts are due February 8, 2019; full applications are due February 22, 2019.
To be considered, domestic applicants must be investigators who have received their terminal degree (e.g., MD, PhD, etc.). For international applicants, current MD, PhD, and MBChB students may apply, along with individuals who have already graduated with their terminal degree. Please see the program solicitation for full details regarding eligibility requirements.
The HPTN Scholars program is funded through a supplement from the U.S. National Institute of Allergy and Infectious Diseases, the U.S. National Institute for Mental Health and the U.S. National Institute on Drug Abuse.

NMAC’s third annual Biomedical HIV Prevention Summit was held on December 3-4, 2018 at the J.W. Marriott in downtown Los Angeles, packed with engaging plenaries, educational breakout presentations, and robust conversations about relevant topics including the #MeToo movement, U=U, intersectionality, PrEP and more. You can see the full agenda with presenters and presentations here: 2018 Biomedical HIV Prevention Summit - Program
Members of our staff including Isabelle Chu and Damilola Jolayemi and members of our Community Advisory Board (CAB) including Luckie Alexander-Fuller, Brandon Harrison, Ace Robinson, Abad Lopez, Damone Thomas, Ricky Rosales were in attendance. We also had members of our faculty and CAB that presented at one of the many workshops and the closing plenary at the conference!
Next year, the Summit will be held in Houston from December 2-3, 2019. For more information, visit the Biomedical HIV Prevention Summit website.
Check out some of our photos below and our live tweets from the event!


We’re at the the Biomedical HIV Summit this morning for the last day of this conference and kicking it off with @PreventionAC for U=U. pic.twitter.com/fHnOKlBxRl
— UCLA CHIPTS (@CHIPTS) December 4, 2018
“This graph speaks for itself”
Rising number of US Syphilis cases juxtaposed with the decreasing federal funding (STD Prevention Budget). #2018BHPS pic.twitter.com/zDkFDXsd16
— UCLA CHIPTS (@CHIPTS) December 4, 2018
“Evidence that there is some risk compensation w/use of PrEP…more routine check ups so STDs are identified more often/people with STDs are more often referred to PrEP.”
“Good news: more check ups for those on PrEP means possibly identifying and treating STDs earlier.” #2018BHPS pic.twitter.com/3v2pFoiHua— UCLA CHIPTS (@CHIPTS) December 4, 2018
Are you a CHIPTS member and have photos from the conference you’d like to share? Send them to chipts@mednet.ucla.edu!

The National Drug Early Warning System (NDEWS) recently released a report on Los Angeles County titled “Los Angeles County, Sentinel Community Site (SCS), Drug Use Patterns and Trends, 2018.” Below you will find the highlights of this report.
To read the full report, you can download a full pdf version here: Los Angeles County Sentinel Community Site (SCS) Drug Use Patterns and Trends (2018) - Report
Highlights
By Mary-Lynn Brecht, Ph.D. UCLA School of Nursing and UCLA Integrated Substance Abuse Programs
A message from CHIPTS
The past year has brought great excitement and hope for the end of the AIDS epidemic in our lifetimes. Global HIV incidence is declining with improvements in ART scale-up, exciting progress to the prevention and treatment cascade metrics, and deployment of PrEP in targeted most-at-risk populations. However, we must not be complacent, as these benefits are not shared equally by all. There is still much more work to be done.
There is an ongoing HIV outbreak occurring among people who use injection drugs in the U.S. The HIV outbreak in Scott County Indiana in 2015 that was linked to sharing injection equipment was not a chance convergence of unique circumstances in a rural part of the country. Instead it was a sentinel event followed by several HIV outbreaks among people who use injection drugs – often opioids. Sadly, a common thread among these outbreaks is that they all occurred in jurisdictions where policymakers (and the citizens they serve) have chosen to limit or to prevent needle and syringe exchange, to not facilitate access to HIV care, and to discourage access to opioid substitution therapy.
We, as citizens and curators of the public health mission, must cry out that this is unacceptable. We know well what is needed to prevent HIV transmissions among people who use injection drugs in the U.S. and globally. We must demand for focused resources and effective policies that support consistent and simultaneous (1) access to sterile injection equipment, (2) access to antiretroviral therapies and (3) access to opioid substitution therapy. Research evidence has shown that these interventions virtually eliminate HIV transmission by:
On this World AIDS Day, it becomes ever clearer that HIV prevention is less underpinned by scientific discoveries than by political will. We must demand for policies that will ensure sustained and equitable access to effective methods to prevent new HIV transmissions. We can, and we must do this for ALL of us – especially for those who face addiction, stigma, discrimination, homelessness, and poverty. Let us enter the new year galvanized, energized, and determined to contribute to moving the HIV incidence needle in Los Angeles, nationally and globally – for ALL.

Image source: Yale Medicine
Abstract: In North America, opioid use and its harms have increased in the United States and Canada over the past 2 decades. However, Mexico has yet to document patterns suggesting a higher level of opioid use or attendant harms.
Historically, Mexico has been a country with low-level use of opioids, although heroin use has been documented. Low-level opioid use is likely attributable to structural, cultural, and individual factors. However, a range of dynamic factors may be converging to increase the use of opioids: legislative changes to opioid prescribing, national health insurance coverage of opioids, pressure from the pharmaceutical industry, changing demographics and disease burden, forced migration and its trauma, and an increase in the production and trafficking of heroin. In addition, harm-reduction services are scarce.
Mexico may transition from a country of low opioid use to high opioid use but has the opportunity to respond effectively through a combination of targeted public health surveillance of high-risk groups, preparation of appropriate infrastructure to support evidence-based treatment, and interventions and policies to avoid a widespread opioid use epidemic.
You can find the full paper here or click this link to download: [Download not found]

Our Center Director Dr. Steve Shoptaw moderated an event by the Los Angeles World Affairs Council titled “The American Opioid Crisis: A Discussion with Chris McGreal, Author of American Overdose” in Culver City on November 28th. Check out the summary from the event below!
This article originally appeared on the Los Angeles World Affairs Council (LAWAC) website. You can see the original article here.
Last year, thousands of Americans died from overdosing on prescription painkillers. The issue, says Guardian journalist and author Chris McGreal, is not just misuse, but over-prescription by doctors and a lack of proper regulation by the US Food and Drug Administration (FDA). McGreal was joined in conversation by UCLA professor and psychologist Steven Shoptaw.
The prescription epidemic started when big pharmaceutical companies successfully convinced medical boards and hospitals to include pain as a vital sign and that it had to be treated as a primary issue, opening the door for over-prescribing. Doctors are now pressured by hospital ethics committees to over-prescribe since being pain free is seen as a human right. On top of that, doctors often learn how to prescribe for a drug from the instructions that come with it, which are written by the marketing departments of drug companies, not by physicians. “Opioids are now the default treatment for pain no matter how weak or strong it is.”
When addicts are no longer able to get what they need from a doctor, they often turn to the black market, where the drugs are often provided by the cartels. The cartels realized they could acquire fentanyl from China, where it is manufactured legally, much cheaper than growing poppies to produce heroin and other opioids. As expected, there is little quality control and batches often contain a mixture of fentanyl cut in with other dangerous drugs, creating extremely lethal concoctions.
Another major influence on the opioid epidemic is the relationship between the FDA and big pharmaceutical companies. “Nearly 60 percent of the FDA’s funding comes from drug companies.” This financial reliance has fundamentally changed the way the FDA regulates medications, and they have frequently approved drugs that their physician and scientist advisory board has denied in the name of an open and fair market.
In October 2017, the Trump administration declared the opioid crisis a Public Health Emergency under federal law. Last month, President Trump signed the Support for Patients and Community Act with wide support from Congress and advocacy groups. The legislation takes aim at the crisis in a variety of ways including curbing shipments of opioids like fentanyl from entering the country, expanding Medicare coverage for treatment and freeing up the National Institutes of Health to conduct more research into non-addictive painkillers.
To read more about the opioid crisis, you can purchase a copy of McGreal’s new book American Overdose by clicking here.
Presented at HIVR4P 2018 – (OA15.06LB) Tail-phase Safety, Tolerability and Pharmacokinetics of Long-acting Injectable Cabotegravir in HIV-uninfected Individuals: HPTN 077 Final Results
Raphael J Landovitz, Sue Li, Joseph J Eron, Beatriz Grinsztejn, Halima Dawood, Albert Y Liu, Manya Magnus, Mina C Hosseinipour, Ravindre Panchia, Leslie Cottle, Paul Richardson, Mark A Marzinke, Susan H Eshleman, Ryan Kofron, Adeola Adeyeye, David Burns, Alex R Rinehart, David Margolis, Marybeth McCauley, Craig W Hendrix
Background: Long-acting injectable Cabotegravir (CAB LA) is an INSTI in development for PrEP. HPTN 077 evaluated CAB LA 800 mg intramuscular (IM) injection every 12 weeks (Q12W) and 600 mg IM every 8 weeks (Q8W) after an initial 4-week interval. Prolonged exposure (the pharmacokinetic [PK] “tail”) after terminal injection results from slow absorption from the injection site depot.
Methods: HPTN 077 was a Phase 2a multicenter study in low-risk HIV-uninfected males and females at 8 sites in Brazil, Malawi, South Africa, and the US. 199 participants were randomized 3:1 to CAB or placebo (PBO) and received oral CAB 30 mg or PBO daily for 4 weeks followed by 800 mg Q12W IM (Cohort 1 [C1], 2x2mL, n=82) or PBO (n=28), or 600 mg Q8W IM (Cohort 2 [C2], 1x3mL, n=69) or PBO (n=20) over 41 weeks. Participants were followed for 52-76 weeks after the final injection for evaluation of adverse events (AE), tolerability and PK.
Results: Retention was 91% and 95% (C1 and C2) at 52 weeks after last injection, and 92% and 93% (respectively) at 76 weeks. Overall in the tail phase, grade 2 or higher AEs were reported by 91% of CAB recipients (87.8% in C1; 95% in C2), compared to 69.8% of PBO participants (76% in C1; 61.1% in C2). Geometric means of apparent terminal half lives (T½app) for males and females will be presented. T½appsignificantly associated with sex and BMI with 1.5 times higher in females than males (p=0.009) and 1.02 times higher per unit BMI increase (p=0.01). Detectable plasma CAB (>25ng/mL) results 52 weeks and 76 weeks after the last injection bye cohort and sex will be presented.
Conclusions: Exposure to decreasing CAB plasma concentrations following the last injection was well tolerated. The T½app of CAB LA for females was significantly increased compared to males. In at-risk persons who discontinue CAB LA, the PK tail phase may represent a period of risk for selection of CAB-resistant virus should HIV infection occur. Data from ongoing Phase 3 studies will help evaluate this risk.